Knee Deep
Geplaatst op 14-04-2024
Intro.
With decades of experience under my belt as an avid roller skate and martial arts practitioner, instructor and having worked with literally thousands of people from all over the world in the capacity of professional trainer, I have witnessed a lot of accidents and injuries and I`ve seen a lot of situations impacting people’s lives in dramatic ways. My field of expertise is human locomotion with a special focus on biomechanical behaviour on roller skates. From this wealth of knowledge, established through education, collecting anecdotal data, grinding through scientific research and practical experience, my work is dedicated to make roller skating accessible in a fun and funky way, with both safety and efficiency as top priority.
In the late 1980’s, I started taking notes on my own personal skill development and my observations of other roller skaters. In 2002, going through a process of rearranging these notes, the first draft of a learning system came to light. Today, the Soulful Fitness Roller Skate Training system has proved itself to be a very effective way, to safely learn roller skating skills. By learning through the system, it becomes a source to assist in extending a Soulful Journey for as long as one’s faculties can keep up, to enjoy that incomparable feeling of freedom in flow. I sincerely hope, this knowledge adds value to your skill.
KNEE DEEP. April 2024
Knee-deep; adjective 1. Up to your knees 2. Very involved in a difficult situation or large task.
(Not just) Knee Deep; a funk classic and second track on the 1979 album Uncle Jam Wants You, by Funkadelic.
As the human body works as a very sophisticated and fully integrated entity, it’s foolish to point out a single part that would be considered crucial for going through our day to day habits and activities. But I do think it’s safe to say, that the health status of our kneejoints are a pretty significant factor in determining the overall quality of an active life and the will and possibillities of having one, for as long as possible.
Since the early 1980’s I have encountered many people doing various sports, that had to change frequency and intensity, due to knee issues. Some even had to step away and quit forever, doing what they loved. In those days knowledge, digital imaging like MRI scans and physiotherapeutical treatments, were definitely on a different level than today (2024), but the human body hasn’t changed at all and human behavior, well – let’s just say it’s quite a challenge to adapt to the spirit of time.
When parts of the human locomotive system start to malfunction for whatever reason, the entire body is involved in trying to compensate for that altered situation. Depending on the severity and nature of the situation – permanent change or temporarily - compensation patterns and postures are manifested in various levels and more than often, totally unconscious. Initially, compensations are meant to relieve the effected / damaged area, so the body can start optimal healing processes. But if the healing process takes too long or those compensations start to get dysfunctional, misalignment stemming from those compensations can cause serious problems elsewhere.
KNEE FACTS.
First, let’s clear some facts considering the knee joint, so that we‘re all on the same page here.
- The knee is the biggest joint in the human body. Although mainly considered a hinge joint, with the main purpose of flexion and extension, there is a slight degree of (medial and lateral) rotation integrated as well, which is a crucial element for optimal functionality of the joint.
- A lot of different structures are involved around and as part of the entire joint, so that means a lot of different types of tissue, such as muscles, tendons, ligaments, connective tissue and cartilage/synovial membranes.
- Problems can be caused due to genetics, excessive overload, inappropriate movement/use and dysfunctional posture.
- The way plates are mounted underneath roller skate boots can significantly influence stance, posture, movement and injury risk.
- Most common injuries with (ice- and) roller skaters are muscle imbalances, tissue tears and patellofemoral syndrome.
MAIN KNEE ISSUES.
Generally speaking, there are four major issues that can not only hinder fluent skill development, but can also cause serious physical obstruction and injuries.
- Leaning forward;
- Bending the knees as a baseline posture;
- The impossibility to flex the toes and the footsoles in a skate boot.
- Inappropriate boot fit.
LEANING FORWARD.
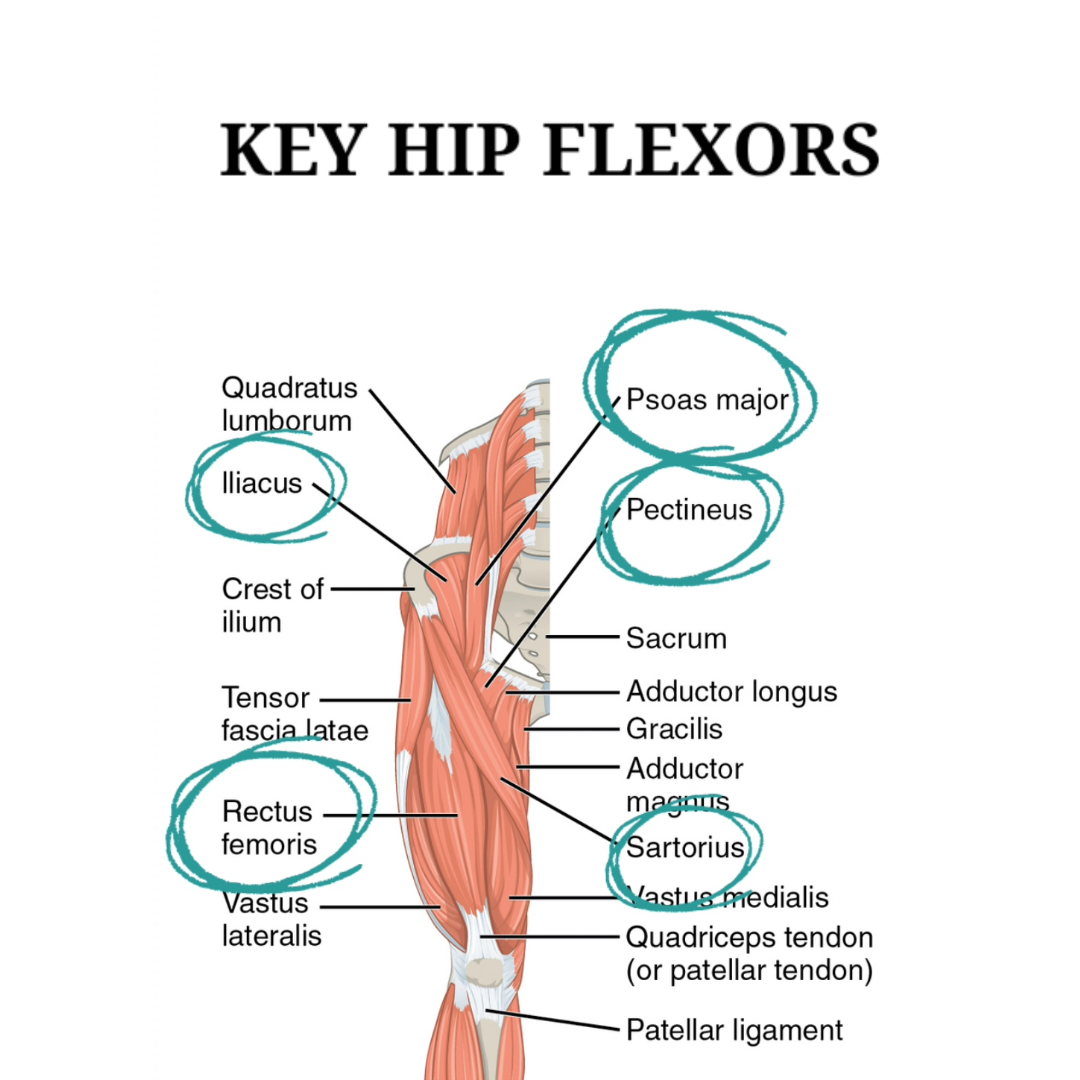
Leaning forward is a very common - and in most cases very unconscious - compensation posture, mostly stemming from the following fear: falling backwards. Another reason often seen is tightness of the hipflexors, due to prolonged sitting. When the leaning forward posture position is not adressed and corrected in the early stages of skill and functional posture development, it has proven to be extremely hard to adjust the trainee into a better position.
Over time, the frontal tilt feels as a straight upright position. In fact, when proper alignment is initiated with someone who is very much accustomed to that frontal tilt, adjustment to a straight upright position where the shoulders are brought right above the (rear) heel, feels to that person as if the person could flip backwards any moment.
Apart from objective correct body alignment and the subjective feeling of standing up straight, leaning forward (frontal tilt) can cause a boatload of issues:
- Ineffective posterior chain engagement. The main musclegroups of the posterior chain are the calves, the hamstrings, the glutes, the erector spinae, the lats (latissimus dorsi), the traps (trapezius) and all the shoulder blade stabilizers. That’s quite a lot, but they are all important to assume a strong and stable upright position.
- With leaning forward usually comes slouching shoulders; especially when the arms are hanging down. Slouching has the effect of compressing the chest and therefore the lungs, making it difficult to inhale properly. Bringing the arms up and the hands above the waistline, opens up the chest and retracts the shoulder blades. In this way, the blades act as shields to keep the upperbody straight up, fierce and engaged. This upright position also makes it easier to engage the abdominal muscles and especially the obliques, to prevent the upperbody from unwanted turns and rotations.
- Leaning forward leads to the very natural and innate reflex of squeezing the toes and footsoles. Try this: stand on your bare feet in parallel position and slowly but gradually lean forward; watch your feet and notice when they clinch and feel when the soles contract. Then try the same exercise with the feet in slightly staggered position. There is really only a very limited degree of leaning forward needed in both situations, before you start gripping the floor with your feet and especially the toes, to keep yourself from falling over. With skates on, you cannot see your feet. But the same reflexes are in effect, even with a very light and slight frontal tilt. On wheels, it’s quite common for people to cramp up at any given moment, up to the point they have to take their skates off to release the cramp; some people get used to it, but often experience fatigued calves, tight footsoles etc. after a certain time of skating; getting used to the frontal tilt position and not experiencing any discomfort, doesn’t necessarily mean you’re off the hook. Eventually a price has to be paid for misalignment and the inevitable manifested compensations. Your body keeps the score and will settle with you, if not sooner, then later.
- Leaning forward as a baseline position builds up pressure in and around the kneejoint. Chances are the hamstrings will get tight over time and other muscle groups have to compensate for that, causing imbalances in the kneejoint, inflammation and imbalances in and between musclegroups, all leading to a higher risk of various types and severity of kneepain. Experiences of burning shins are also very common, caused by excessive stress on the shin muscle (tibialis anterior), due to excessive muscle overload as a result of leaning forward (overcompensation).
- The frontal tilt makes it difficult to push and tilt the pelvic area forward and lock this position. The purpose of this lock is to control the upperbody and to prevent unnecessary and counterproductive swaying and swinging. Not being aware of the benefits of locking the pelvis, makes roller skating – especially for beginners – so much harder than it has to be. And the chance of either falling forward or backwards increases massively. Locking and unlocking the pelvic area at will and with purpose, opens up the door to deliver spice and personal touch to roller skating skills.
 BENDING THE KNEES.
BENDING THE KNEES.
Bending the knees as a baseline posture is common advice heard and spread around the skating world. Unfortunately it is very bad advice, without any validated arguments. The most common reason why people are told to bend at the knees, is to prevent them from falling backwards as soon as the skates move in any direction. When leaning forward is thrown in the mix as well, the argument is supposed to be, that flipping backwards is not likely to happen when upper body mass is tilted forward.
However, these are all clear indicators of very poor instruction to say the least, based on very little to no understanding of basic biomechanics on roller skates.
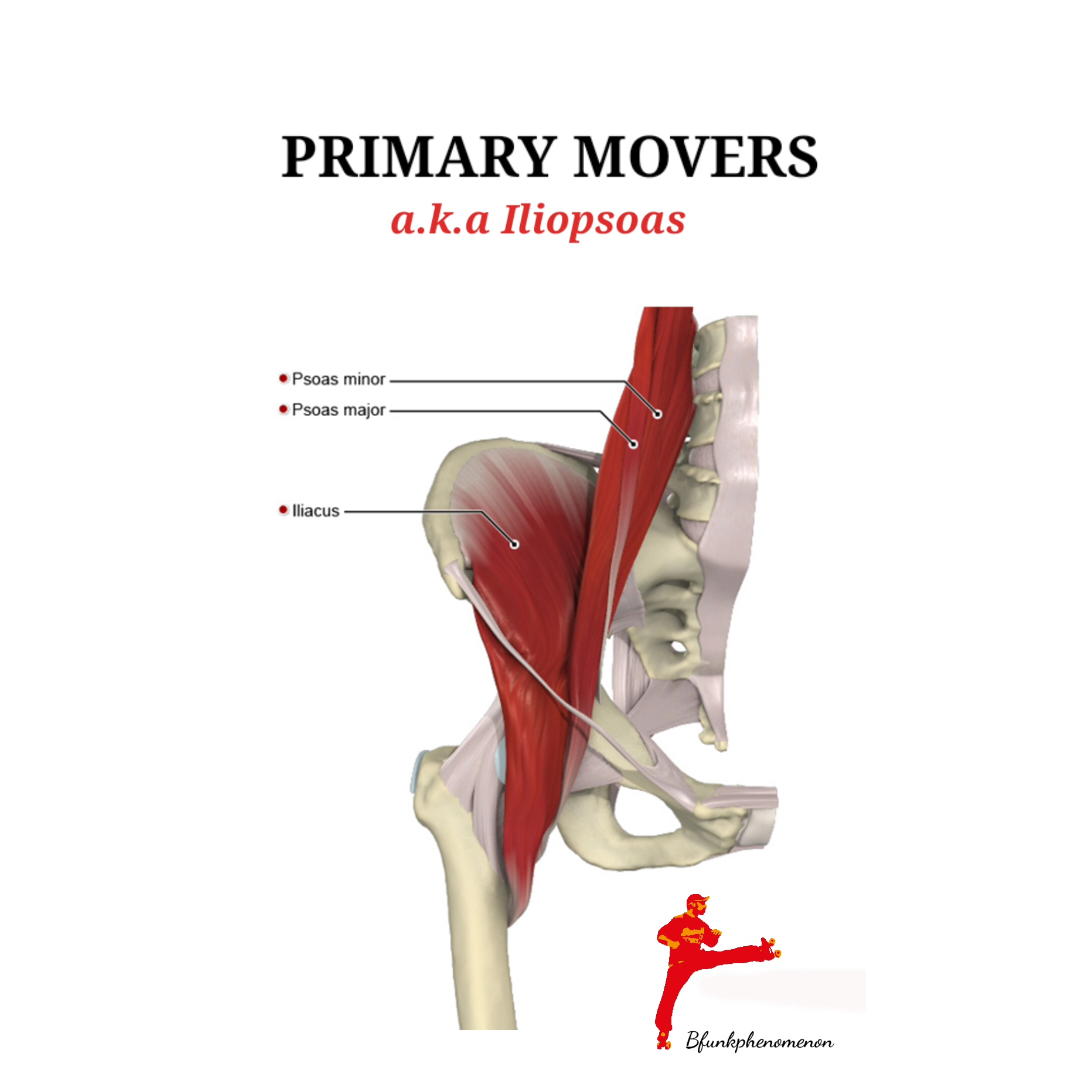 It’s very understandable that you want to prevent people from falling, and especially flipping backwards, where people stretch their arms in order to break the fall and as a result break their wrists, arms, dislocate shoulders and so on, or hitting the back of the head on the pavement and any other horror scenario. But the crux of the matter is, moving and controlling the center of mass when skating upright, is not regulated at the level of the knees; alignment of the body and moving the body as a whole is always managed from the core. The core being, the abdominal muscles and the iliopsoas muscular connection, also known as the primary hip flexors.
It’s very understandable that you want to prevent people from falling, and especially flipping backwards, where people stretch their arms in order to break the fall and as a result break their wrists, arms, dislocate shoulders and so on, or hitting the back of the head on the pavement and any other horror scenario. But the crux of the matter is, moving and controlling the center of mass when skating upright, is not regulated at the level of the knees; alignment of the body and moving the body as a whole is always managed from the core. The core being, the abdominal muscles and the iliopsoas muscular connection, also known as the primary hip flexors.
Controlling the center of mass and managing to move the body as a whole, when rolling (either forward or backwards) requires training and performing exercises, that effectively lead to an acceptable level of safety and comfort. There is no quick fix for this and certainly not at knee level.
For the love of your knees, DO NOT BEND YOUR KNEES. Or put even more accurately: DO NOT KEEP YOUR KNEES BENT AT ALL TIMES.
Bending the knees sure has it’s place and function and when timed correctly, it’s very beneficial to certain techniques and can add flavour and flamboyance to different moves. But there is a lot of misconception about how far the knees should be bent during upright skating and what the margins are for fluent moving around.
Before going knee deeper into the details, it’s important to point out that continuously bent knees, put a lot of strain on frontal elements of the joint, in particular the patellofemoral ligament. Also, bending the knees is usually paired with a frontal tilt. With all the information about the effects of leaning forward in mind, it’s not hard to imagine how the combination of those two forementioned factors can lead to higher chances of yes, wounded knee situations with cumulative effects.
RELEASE & RELAX POSITION.
Time to get really technical and accurate about the position of the kneejoint. Because, if ‘bend your knees’ is inherently bad advice, then what is good instruction and the right angle and degree of bending? And should you have a goniometer on you at all times for the rest of your skating life, to keep yourself and your rolling loved ones safe?
To start with the last question, the answer is no; you don’t need to carry tools and instruments around with you, to be safe. But, awareness of the following is highly advised:
- A full straight knee position means, there is zero degree of bending and the upperleg muscles (aka quadriceps or quads) are fully engaged and contracted, and the joint is totally locked. Mind you, this is a deliberate lock, not to be confused with a pathologically caused lock, which in all cases is quite painful. During the last portion of knee extension ( approx.30 degrees) there is a slight rotational mechanism in the kneejoint activated, which is the so-called ‘screw-home mechanism’. This slight torque movement is essential for healthy knee action. In other words: rotation is a must to fully achieve extension and any degree of flexion from full extension.
- Relaxing the quads and contracting the popliteus muscle unlocks the knee from the forementioned deliberate locked position.This position is what I refer to as the Release & Relax phase (RR position). Technically, this results in anywhere between 2 to 10 degrees of knee flexion. This minimal movement of flexion hardly puts stress on any part of the knee joint and in particular both the patellar ligament and the quadriceps tendon are spared considerably. The popliteus muscle is crucial in the initial phase of knee flexion, assists in releasing the screw-home-mechanism, has a significant role in control of hyperextension of the kneejoint and is therefore refered to as the ‘key of the knee’, which also entails a key role in the RR position.
- From approximately 10 degrees knee flexion on, is where stress starts to accumulate, effecting the tendons and ligaments attached to the knee cap (patella). A young healthy knee can take a lot, but even then, assuming a flexed postion of ten degrees or more for an extended period of time on a regular basis during any sports activity, is an impactful and more than often degenerative habit for most kneejoints in any sport or occupation.
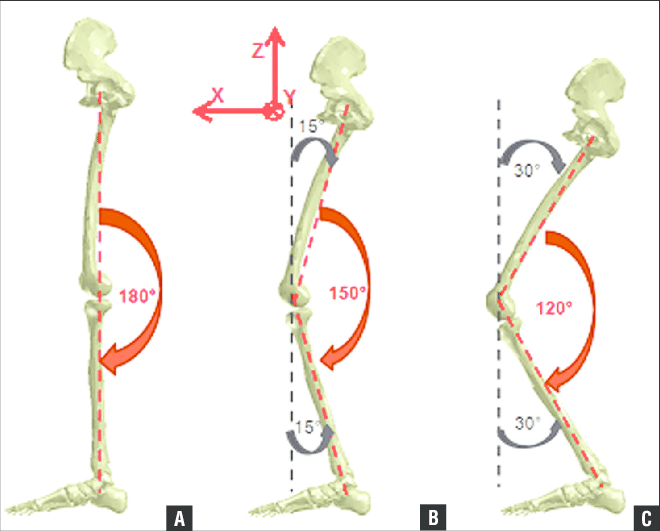 To put all this in perspective, the following illustration shows upright knee flexion in different positions:
To put all this in perspective, the following illustration shows upright knee flexion in different positions:
- 0 degrees;
- 30 degrees knee flexion;
- 60 degrees knee flexion.
Instructing people to assume position C in basic upright roller skating, while position B is already too far bent, is a straight forward assault on the knees. For safe and efficient skill development with fluent transitions, all basic roller skating skills are practiced with knee flexion in the range of 5 to a maximum of 20 degrees, depending on the technique. (Up to max. 10 degrees flexion is the RR position, as described earlier in this article. In our training sessions, we also refer to the RR-position as `soft knees`.)
The illustration below pictures a good reference of general active range of motion (AROM) when flexing the knee, with only the lower leg changing position.
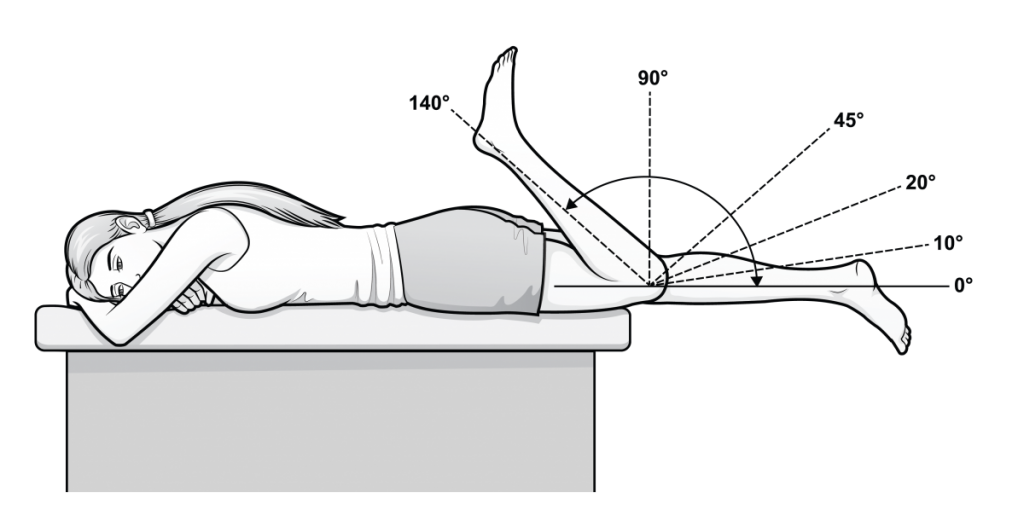
* Normal range of motion is usually between minus 6 to 143 degrees. When the heel is pushed or pressed towards the buttocks (passive range of motion), there is even more than 145 degrees flexion possible.
In our Soulful Fitness Roller Skate Training sessions, we never adress the position of the knees in such a way, where we ask or tell people to `bend the knees`. We always explain the exact position of the knees and refer to this position as `relax the knees`, or `be mindful of the soft knee position`. This is even more important when a trainee has existing knee lesions, or a history of knee problems. Words, terminology and the exact meaning all matter; not leaving any room for confusion and discrepancy, keeps people safe and out of harm’s way. It also equips them with good guidance and safe information, when they are practicing on their own and share what they have learned with other roller skate lovers.
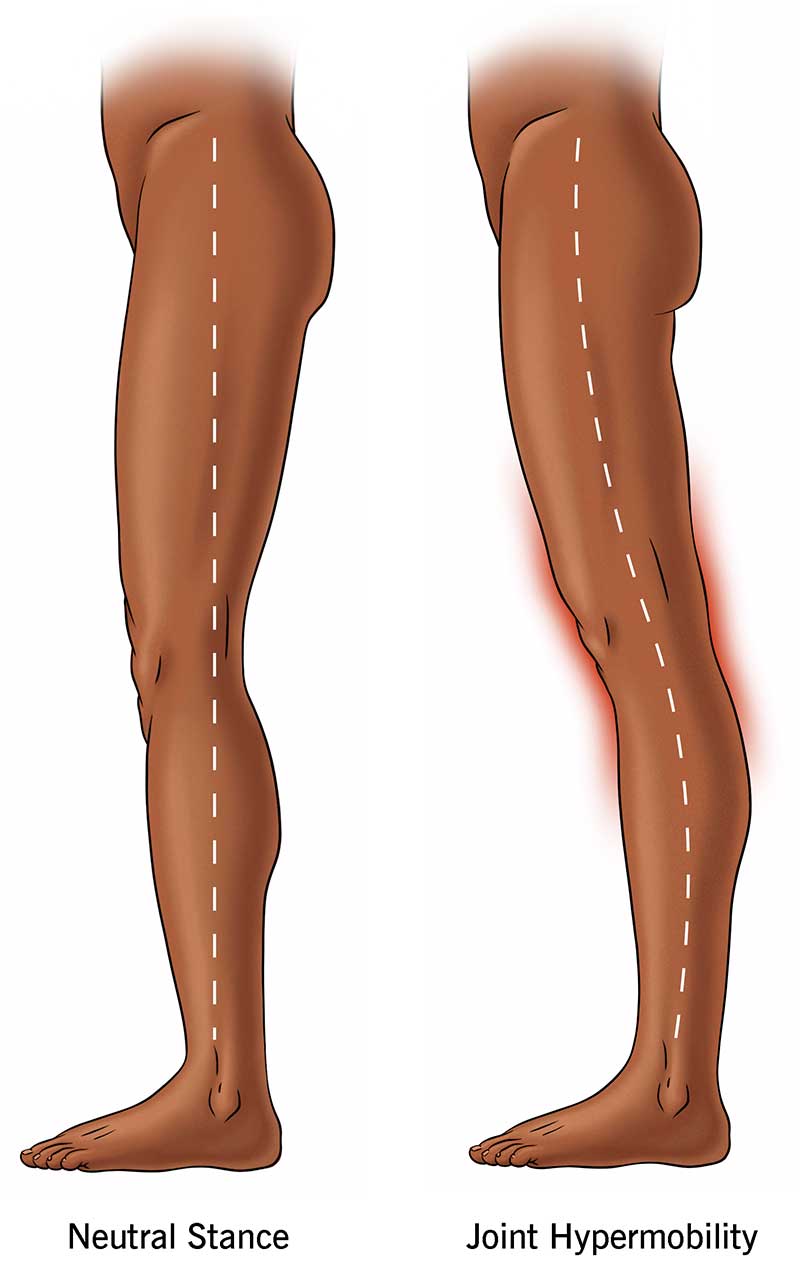 JOINT HYPERMOBILITY.
JOINT HYPERMOBILITY.
Flexibility of joints is a good thing and hypermobility is very common and not initially something to worry about when lacing up roller skates. But if the flexibility range goes into extreme negative numbers accompanied with pain and other symptoms, caution and good instruction more mandatory than a luxury. A genetic condition called joint hypermobility syndrome could be at play, which usually doesn’t involve just one joint. The knee joints however, are very prone to this condition. The syndrome is mainly considered a connective tissue disorder, where the joint capsule and attached ligaments are weakened and lose their elasticity to keep the joint compact and all parts in place, also effecting muscle tone of surrounding muscles.
There is not a straight forward solution for painful hypermobility, but a safe individualized strength training program can manage the situation and effects very well. When roller skating, hyperextension of the knees should always be avoided and of course the degree of knee flexion should be monitored very closely. Unusual hypermobile knees are a good indication, for possible ongoing issues elsewhere in the body. Problematic control of pelvic tilt and an arched spine, are common problems among roller skating practitioners. When these issues are identified in practice, it’s important to keep in mind, that the particular trainee already has developped compensation patterns, from living day to day life. Any type of adjustments needs to be adressed carefully and roller skating exercises and techniques should always be modified accordingly. That said, roller skate practice can have very interesting therapeutical value to gain or regain total body awareness.
THE IMPOSSIBILITY OF FLEXING AND STRETCHING THE TOES.
Flexing and stretching (pointing) the toes is essential for good stability, generating forward motion and shock absorption. Not being able to use full range of motion and functionality means joints, muscles and tendons upstream have to compensate for the inability to fully move the toes.
It is literally impossible to stand on your toes and experience full feet-functionality, when wearing roller skate boots. Immobilization of the feet for an extended period of time on a regular basis has a big impact on the whole body, as it effects the entire kinetic chain upstream.
Therefore, it is extremely important to spend significant time on activities that involve flexing and stretching the toes, to literally counter the effects of prolonged immobilization, due to limitations of a classic roller skate boot. Mind you, it’s not necessarily the boot’s fault; it’s of course the plate mounted underneath, that makes the structure rigid. So time spent off-wheels adressing flexing, stretching and strengthening the feet is key.
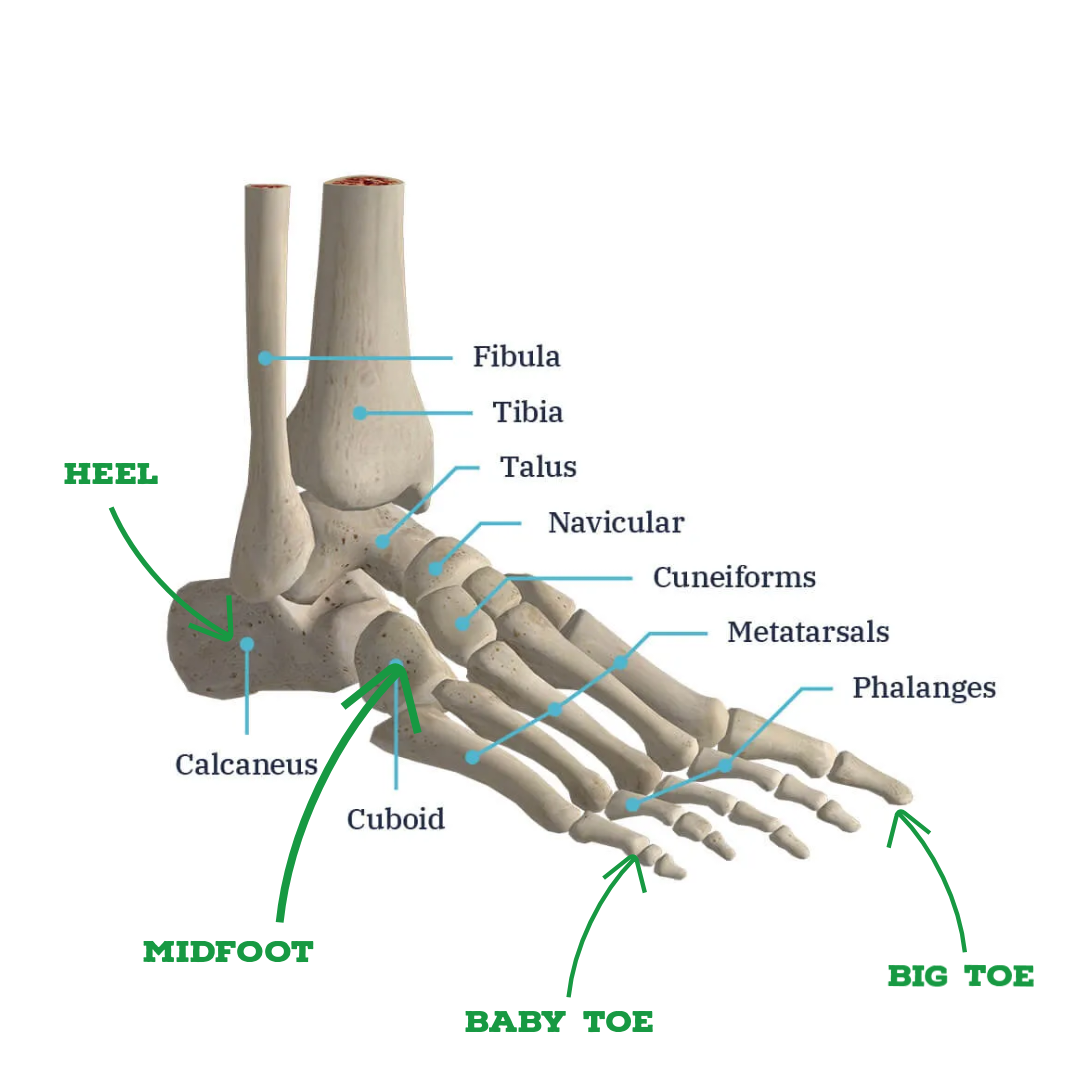 Especially the big toe (hallux) is a big player for proper biomechanics and the metatarsal head is one of three pillars of the foot; the other two being the heel and the metatarsal head of the baby toe. When zooming in on biomechanical level in normal walking, the big toe acts as a springboard to push off the ground. When descending or stepping down, the metatarsal joints of the feet absorb approximately 86% of all bodyweight, of which the the biggest portion at the expense of the big toe. Now taking away these major functional tasks by immobilizing the feet, automatically means changes in biomechanical function and the way shock is absorbed upstream by joints and connective tissue. So keeping your feet and big toe fit and functional off-wheels is an absolute must.
Especially the big toe (hallux) is a big player for proper biomechanics and the metatarsal head is one of three pillars of the foot; the other two being the heel and the metatarsal head of the baby toe. When zooming in on biomechanical level in normal walking, the big toe acts as a springboard to push off the ground. When descending or stepping down, the metatarsal joints of the feet absorb approximately 86% of all bodyweight, of which the the biggest portion at the expense of the big toe. Now taking away these major functional tasks by immobilizing the feet, automatically means changes in biomechanical function and the way shock is absorbed upstream by joints and connective tissue. So keeping your feet and big toe fit and functional off-wheels is an absolute must.
INAPPROPRIATE BOOT FIT.
It’s not easy to find the right boot for your style or preference of roller skating. A good fit is the most important issue that matters, but unfortunately distractive forces such as aggressive marketing strategies by companies, social media pressure and peer pressure, fueling the urge to be accepted by (local) skate culture more than often blur honest and unbiased informed decision making and can lead to questionable choices with disappointing outcomes.
So again, a good fit is the most important issue when you have to make a boot choice. The boot model should be functional and conducive to your skating goals. Wrong size, too tight of a fit, too big, heel too high, no heel, too stiff, no support at all, all these variables matter and have an impact on the development of your skate style, technique and physical health and safety. Customizing roller skate boots sounds like a great fashionable and sexy feature, but you can only customize colors and sometimes type of fabric of the boot. The elements that really matter such as heel height, (enough) boot width and stiffness, cannot be changed at all or just partially. So it all comes down to wisely taking an abundance of time to try on as many different boots from different brands as possible.
There are services in place where you can send exact measurements of your feet or send even an entire mold and discuss your preferences for how the boot eventually has to be. If budget is not an issue, it could be an avenue to pursuit, but such a project generally starts from somewhere around 1500 to 2000 (US) dollars and that just covers the basics. Even when a boot gives that ‘perfect fit at first feel’ vibe, still the boot has to prove itself over time. Same goes of course for plates and wheels, but they are much easier to change.
HEELED OR FLAT?
As with almost every aspect of roller skating, the choice for a boot with a heel or a low cut boot or sneaker type model without a heel, boils down to personal preference and to a lesser degree particular style of skating. The total sum of (expected) frequency and goals plus style of skating, leads to the result translated into type of boots, shoes, plates and wheels.
However, in terms of functionality and impact on the body, there are elements which are interesting to be aware of and helpful in order to make a decision. The difference between a heeled and flat sole certainly is one of them. In order to have a good understanding of the difference and impact, I will illustrate this with the mitella analogy.
MITELLA ANALOGY. (recovery of a broken arm, elbow and shoulder issues).
Although the word mitella means female headdress or sling in Classical Latin, in modern days the armsling is used for the recovery of a broken arm and traumas to the elbow and shoulder area. Using a mitella means arm, joints, muscles and ligaments are all positioned in resting position; every structure and tissue involved, when the arm is placed in the mitella is biomechanically brought in the most convenient position for efficiënt recovery with the least amount of energy use.
A heeled boot brings the leg, knee and hips in a similar convenient position in terms of biomechanics, which brings the chance of developping injuries significantly down. A heeled boot has more potential to correct a leaning forward position; a flat sole can easily provoke a forward tilt and have you bend the knees more than necessary.
When flat soled sneaker type skates or low cut boot roller skates are for short or not so frequent rides, they will not have that much of an overall impact, especially when it’s a pair on the side and the focus is more on practicality. When it’s the main setup where the majority of skating time is spent on, you might wanna take the above mentioned info into consideration. Roller skating on a flat sole always involves biomechanical compensations in one way or the other, no matter the duration of your skating time.
MORTON’S NEUROMA.
A very common issue among roller skaters is a condition in the foot developped over time, where tissue around one of the nerves leading to the toes becomes thickened. The consequential inflammation brings sharp and burning pain sensations to the ball of the foot, as well as stings to the toes and even numbness. The major cause is too narrow skates, where the toebox leaves no room for the toes to spread. There are a lot of roller skaters who probably don’t even know they have this condition going on in some degree, in one or both feet. So it’s good to know about symptoms and act in time, before matters get worse. What’s the almost worst thing that can happen besides increasing excruciating pain? Having to undergo surgey. The absolute worst thing that can happen? Not getting rid of the problem, no matter the intervention and as a consequence having to end a blissful and promising skate journey.
BALANCING TIME ON & OFF WHEELS.
So what is the best way moving forward in any situation? Well, on roller skates don’t bend your knees more than the exercise or move requires, but keep `m soft. Keeping your knees within safe margins, means treating them with reverence. Physical exercise off-wheels is highly recommended, not only for longevity in general, but also to empower your skate power.
In one word, Rollgevity: It’s not about how good you roll, but it’s all about how long you roll good. Being mindful of how and how much you tax your knees on a daily basis is a very important part of rollgevity and effective skill development. Specific muscle targeted training, with special focus on glutes and hamstrings can counter muscle imbalances. With compound exercises such as (box) squats and deadlifts, but also hip thrusts, slant board exercises, back hyperextension plus reverse hyperextension, walking backwards and various band-assisted exercises, you can safely and incrementally build the strength and endurance needed for daily life and your skating goals.
Facing the unevitable process of organic degeneration – or simply put, aging – strength training off wheels also slows down aged related effects such as gradual but progressive loss of muscle mass, strength and function (formal medical term, sarcopenia). This can seriously cause muscle imbalances in different parts of the body and the kneejoints are no exception. Moves you’re able to do in your twenties and thirties or you’ve been doing your whole life, are going to feel and hit different in your fifties and sixties and probably need adjustments in intensity and/or range of motion. At a certain point in life, just roller skating is not enough for maintenance.
There`s absolutely no doubt that hitting the weight room will massively improve the quality of your life and keep your skate flow safe and funky for a long time.
REST & RECOVERY TIME.
Resting time is a highly underrated aspect of any training and performance program. And with something as fun as roller skating – especially when it totally gets a hold of you to the point of freaking fanaticism – it’s easy to forget about taking enough rest to recover.
Yes, you want to do all the parties, all the gatherings, all the high profile indoor and outdoor jams and post as much of it on social platforms ‘all day every damn day’, to express how hectically crazy fun skatelife is; you are definitely not alone in this and it’s quite understandable considering the modern day zeitgeist and all that has come with that.
However, it’s in properly balanced resting time with enough quality sleep, where the necessary recovery and adaptation from a solid training program actually takes place. All activities outside of the main training program – considering duration and intensity – need to be added to the total sum of load on the body, mind and soul, in a particular timeframe. But a smart training program is meant as a preparation for all activities you have planned to get yourself into, basically making them a walk in the park.
As stated in the beginning of this article, we all rely heavily on our kneejoints to have smooth days and fun experiences for as long as we can. That means our knees have a lot to endure going from day to day, performing the tasks that we need to do and the goals we set out to pursuit. A high demanding activity such as roller skating, adds to the equation and requires thoughtful planning and a deeper understanding of how to keep yourself in the game.
Also mentioned earlier, the kneejoint consists of a lot of different structures. All these different types of tissue have a different recovery rate, in case of (micro) damage or any kind of lesion, or just simply from being put under load and pressure. In case of any discomfort or pain, it is wise to identify how, when and where exactly in the body or the joint the discomfort is experienced. After appropriate resting time and perhaps consulting a medical professional, closely monitoring the developments will hopefully keep you away from slipping the event into a chronic or life altering situation. Being mindful of taking enough time to rest and digest is the smart way to flow.
In case of consulting a physician, make sure to lay out all of your roller skating endeavours and activities, the time you spend on wheels, how important it is to you and so on, as clearly as possible. In general, they usually don’t have a clue what modern day roller skating is all about, the friction of wheels on different surfaces (creating immense torque action in the knees) the roller skating biomechanics etc. The more you make them understand, you are not a regular civilian but a roller skater (no matter style or discipline) the better they can help you, the better they WILL help you. Whenever you experience continuing discomfort, or suspect an injury, I strongly recommend consulting a healthcare professional for an accurate diagnosis and appropriate treatment plan. And of course, communicate your experiences and findings with whoever your learning with or from; you might save a knee or two.
In today’s world, there is nothing you cannot educate yourself about. The only problem is how to sift through all the available information and separate from misinformation. Regarding the knee, I have compiled a short list of most common knee lesions, that can occur due to wear and tear. A starting point in case of or prevent any issues.
The next step - and I can’t stretch this enough - is to contact a health care professional. Struggling through pain and discomfort is not necessary. Listening to anecdotal experiences and interventions will only take you so far; a professional can offer a safe plan with options which that can be monitored.
The English physician Thomas Sydenham (1624-1689) widely considered as the English Hippocrates, coined the phrase ‘A man is as old as his arteries’. Many centuries later, with advanced research and improved technology, we definitely know all too well that the quality of arteries is a huge determining factor in quality of life. Blood stream, brainwaves, heart rate and so on are all elements that have a certain flow. Movement is extremely important to keep all those different elements flowing in a healthy state. We are as good as the sum of all that makes us flow; as a human being, as a community, as a society, as part of the world.
To summarize my overall advise: train, rest, party & repeat and keep flowing.
Brian B. Kanhai, Soulful Fitness Roller Skate trainer.
A summary of common knee injuries that can occur due to wear and tear:
1. Osteoarthritis: This is a degenerative condition where the protective cartilage within the knee joint wears down over time. It can cause pain, stiffness, swelling, and reduced mobility.
2. Meniscus tears: The meniscus is a rubbery cartilage that acts as a cushion between the thigh bone (femur) and shinbone (tibia). Tears in the meniscus can occur with age-related degeneration or sudden twisting movements, leading to pain, swelling, and difficulty moving the knee.
3. Patellofemoral pain syndrome: Also known as "runner's knee," this condition involves pain around the front of the knee, particularly under or around the kneecap (patella). Overuse, muscle imbalances, or poor alignment between the patella and femur can contribute to this condition.
4. Tendinitis: Tendons connect muscles to bones, and repetitive stress or overuse can lead to inflammation and pain in the tendons around the knee. Patellar tendinitis (jumper's knee) and iliotibial band syndrome (ITBS) are two common types of knee tendinitis.
5. Bursitis: Bursae are small fluid-filled sacs that act as cushions between tendons, ligaments, and bones. Overuse or trauma can cause inflammation of the bursae, resulting in bursitis. Prepatellar bursitis (housemaid's knee) and infrapatellar bursitis (clergyman's knee) are examples of knee bursitis.
6. Patellar dislocation: This occurs when the patella slips out of its normal position, usually towards the outside of the knee joint. It can be caused by sudden twisting movements, direct trauma, or structural abnormalities in the knee. Patellar dislocation leads to severe pain, swelling, and instability.
Potential causes of knee pain, depending on the location.
Knee pain above the knee, potential causes:
- Quadriceps Tendonitis: Quadriceps Tendonitis is a condition associated with irritation, injury, or strain to the quadriceps tendon. This leads to inflammation.
- Patellofemoral Arthritis: Arthritis that affects the underside of the patella or knee cap and the femur groove is known as Patellofemoral arthritis. This is caused by the wearing away of articular cartilage.
- Syndrome of Plica: Plica is the fold of synovial membrane lining the knee joint. When this fold gets inflamed, it can lead to significant pain and weakness above the frontal aspect of the knee.
- Synovitis: Synovitis is associated with the inflammation of the synovial lining of the knee joint. It is mostly caused by overuse.
Pain in the knee, potential causes:
- ACL Injury: ACL, which stands for the anterior cruciate ligament, provides the knee stability and movement control. Like an ACL tear, Ligament tears are a common cause of pain in the knee. It may also be associated with MCL, LCL, and PCL.
- Patellofemoral Pain Syndrome: Patellofemoral pain syndrome is associated with a dull pain in the knee cap or the front of the knee. This may be caused by the displacement of the knee cap or its overuse.
- Patella Chondromalacia: This presents with a grating feeling on movement and pain in the junction of the thigh bone and knee cap.
- Partial Dislocation of Patella: Partial dislocation of the patella may be caused by trauma or twisting of the knee cap. This is often presented with severe pain in front of the knee.
- Tendonitis of Patella: Inflammation of the patellar tendon may be caused by overstretching or extra stress being imposed on it.
- Osgood Schlatter Disease: This condition is commonly encountered by adolescents. It is commonly caused by inflammation at the shinbone and patellar tendon junction.
- Bursitis: Bursitis is associated with inflammation in the fluid-filled sacs in the front of the knee known as Bursae.
- Osteoarthritis: Osteoarthritis affecting the knee joint is another cause of knee pain. This condition is associated with the breakdown of the articular cartilage, which can no longer cushion the bones.
Pain in the back of the knee, potential causes:
- Sciatica- The sciatic nerve runs down the leg behind the knee. It splits into two nerves, the tibial and peroneal branches. It’s common for the sciatic nerve to experience compression from a hamstring strain.
- Baker’s Cyst: Excess fluid buildup at the back of the knee joint can lead to a Baker’s cyst, causing pain and stiffness, commonly from a meniscal tear.
- Hamstring Tendonitis: Inflammation and irritation of the muscles at the back of your thigh responsible for leg extension can result in pain.
- Meniscus Tear: Tears in the cartilage pads within your knee joint, often caused by sudden twists or changes in direction, can lead to discomfort when straightening your leg.
- Posterior Cruciate Ligament (PCL) Injury: Injuries to the PCL at the rear part of your knee may result in posterior knee pain during full leg extension.
- Knee Arthritis: Osteoarthritis or rheumatoid arthritis affecting the kneecap can contribute to discomfort behind the knee during complete extension.
- Popliteal Injury: An external leg rotator that can become injured from overuse or a strength imbalance with the hamstrings.
Pain on the outside of the knee (lateral), potential causes:
- Hamstring Tendinitis: The hamstring tendon connects the hamstring muscle to the back of the knee. This condition is associated with inflammation of this tendon.
- Iliotibial Band Syndrome: Iliotibial band syndrome is caused by inflammation of the iliotibial band that is found between the tibia and pelvis.
- Damage to the Lateral Collateral Ligament: This damage may be caused by a sprain, trauma, or ligament tear.
- Lateral Meniscus Tear: The lateral meniscus is usually crescent-shaped and acts as a shock absorber for the knee joint. The symptoms of its tear include walking difficulty and swelling.
- Posterolateral Corner Injury: The poster lateral corner injury may be caused by trauma due to sporting injuries. This may also be associated with Posterior Cruciate Ligament injury.
- Tibial Plateau Fracture: This is a complex injury that is associated with a fracture of the shinbone or the proximal end of the tibia.
Pain on the inside of the knee (medial), potential causes:
- Medial Meniscus Tear: A tear of the medial meniscus, which is found on the inner side of the knee, can cause swelling, mobility issues, and significant pain. These symptoms are similar to a lateral meniscus tear.
- Damage to the Medial Collateral Ligament: MCL damage is among the most common knee ligament injuries. This injury may present itself in the form of a stretch, tear, or outwards force. Symptoms often include bruising and stiffness.
- Osteoarthritis When the cartilage of the medial femorotibial compartment wears down, the extra synovial fluid can create bony osteophytes. This causes the bones in your joints to rub together.
- Avascular Necrosis: Avascular necrosis, also known as osteonecrosis of the knee, is a painful condition that occurs when the bone tissue dies due to a lack of blood supply, causing the bone to collapse. It can often be attributed to heavy alcohol or long-term steroid medication use.
References.
Abulhasan, J.F.; Grey, M.J. Anatomy and Physiology of Knee Stability. J. Funct. Morphol. Kinesiol. 2017, 2, 34.
Lubowitz JH, Bernardini BJ, Reid III JB. Current concepts review: comprehensive physical examination for instability of the knee. The American journal of sports medicine. 2008 Mar;36(3):577-94.
DOOLEY NOTED: Popliteus Muscle Location for Knee Pain. Available from: http://www.youtube.com/watch?v=zO95xFvEVG4
Popliteus Muscle - Origin, Insertion, Function & Innervation - Human Anatomy | Kenhub. Available from: http://www.youtube.com/watch?v=X7xbuAN2XDk
Hall, S. J. (2015). Basic biomechanics (7th ed.). New York, NY: McGraw-Hill Education.
Palastanga, N., & Soames, R. (2012). Anatomy and human movement: structure and function (6th ed.). Edinburgh: Churchill Livingstone.
Lippert, L. S. (2011). Clinical Kinesiology and Anatomy (5th ed.). Philadelphia, PA: F. A. Davis Company.
Standring, S. (2016). Gray's Anatomy (41st ed.). Edinburgh: Elsevier Churchill Livingstone.
The Effect of Mechanical Varus on Anterior Cruciate Ligament and Lateral Collateral Ligament Stress: Finite Element Analyses. April 2016 Orthopedics 39(4):1-8 DOI:10.3928/01477447-20160421-02
Explosive strength: effect of knee-joint angle on functional, neural, and intrinsic contractile properties. Marcel Bahia Lanza, T G Balshaw , J P Folland PMID: 31115654 PMCID: PMC6647239 DOI: 10.1007/s00421-019-04163-0
The foot as a shock absorber. E P Salathé Jr 1, G A Arangio, E P Salathé PMID: 2384481 DOI: 10.1016/0021-9290(90)90165-y
A biomechanical model of the foot: the role of muscles, tendons, and ligaments. Salathe EP, Arangio GA.J Biomech Eng. 2002 Jun;124(3):281-7. doi: 10.1115/1.1468865.PMID: 12071262
Functional anatomy and imaging of the foot. Ridola C, Palma A.Ital J Anat Embryol. 2001 Apr-Jun;106(2):85-98.PMID: 11504250 Review.
A Bio-Inspired Arched Foot with Individual Toe Joints and Plantar Fascia. Burgess S, Beeston A, Carr J, Siempou K, Simmonds M, Zanker Y.Biomimetics (Basel). 2023 Sep 26;8(6):455. doi: 10.3390/biomimetics8060455.PMID: 37887586
Investigating the Effect of Aging on the Viscosity of Tendon Fascicles and Fibers. Karathanasopoulos N, Ganghoffer JF.Front Bioeng Biotechnol. 2019 May 15;7:107. doi: 10.3389/fbioe.2019.00107. eCollection 2019.PMID: 31157219